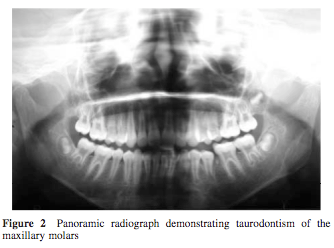
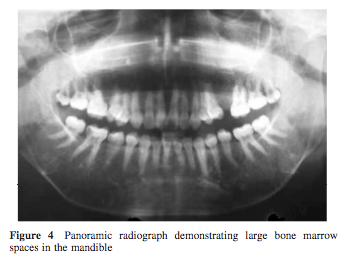
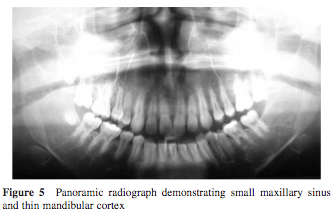
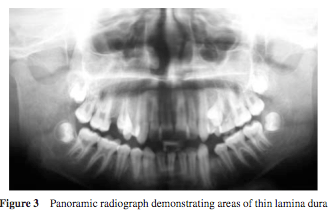
Panoramic Radiographic sign in Thalassemia patient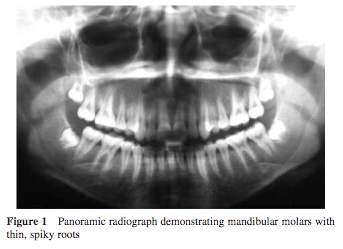
08 October 2008
19 April 2008
Erythropoietin definition
Erythropoietin (EPO): A hormone produced by the kidney that promotes the formation of red blood cells in the bone marrow. EPO is a glycoprotein (a protein with a sugar attached to it). Human EPO has a molecular weight of 34,000.
The kidney cells that make EPO are specialized and are sensitive to low oxygen levels in the blood. These cells release EPO when the oxygen level is low in the kidney. EPO then stimulates the bone marrow to produce more red cells and thereby increase the oxygen-carrying capacity of the blood.
Dental Consideration in Chronic renal failure
ผู้ป่วย Chronic renal failure มักจะต้องได้รับการ hemodialysis ซึ่งจะมีการทำ Arteriovenous fistula ด้วย Prosthesis ไว้ ก่อนรักษาทางทันตกรรมที่ก่อให้เกิดเลือดออกจึงควรให้ Antibiotic prophylaxis ด้วย และ renal ยังเกี่ยวข้องกับการสร้าง red blood cell และ white blood cell ด้วย
ผู้ป่วยที่ต้องทำ hemodialysis มักต้องทานยาพวก warfarin หรือฉีด heparin จึงควรประเมินภาวะ bleeding ก่อนทำหัตถการ โดยมักทำหลังจาก hemodialysis 1 วันเนื่องจากหมดฤทธิ์ของยาห้ามเลือด(heparin half-life 90 min) และทำให้แผลหายเร็วกว่า ป้องกันการติดเชื้อ(เนื่องจากเลือดพึ่งฟอกเสร็จ ประสิทธิภาพในการ healing ก็จะดีกว่า)
Chronic renal failure จะทำให้มีการสร้าง Vitamin D ไม่เพียงพบ ซึ่ง Vitamin D ทำหน้าที่ดูดซึม Ca2++ จากลำไส้เล็ก ถ้าขาด Vit D จะทำให้เป็น secondary hyperparathyroidism ทำให้กระตุ้นให้สร้าง parathyroid hormone มากขึ้นเพื่อเพิ่ม Ca2++ ในเลือด จึงทำให้ metabolism ของกระดูกเปลี่ยนไปเนื่องจากไปดึง Ca2++ ออกจากกระดูก(bone resorption)
ดังนั้นผู้ป่วย chronic renal failure มักจะเกิดร่วมกับ secondary hyperparathyroidism ซึ่งจะทำให้เกิดปัญหาของการสร้างกระดูกหลังถอนฟันได้ (ในผู้ป่วยอายุน้อยที่เป็น chronic renal failure มักจะมีรูปร่างเล็ก ฟันไม่ขึ้นตามอายุ ก็เนื่องจากสาเหตุนี้เช่นกัน)
13 April 2008
Antibiotic Prophylaxis in dental procedure (2007)
การให้ Antibiotic เพื่อป้องกัน IE (Infective endocarditis) ของเมื่อปี 1997 จะให้ในผู้ป่วยที่มี underlying disease ดังนี้
- mitral valve prolapse
- rheumatic heart disease
- bicuspid valve disease
- calcified aortic stenosis
- congenital heart conditions such as ventricular septal defect, atrial septal defect and hypertrophic cardiomyopathy.
- artificial heart valves
- a history of infective endocarditis
- certain specific, serious congenital (present from birth) heart conditions, including
- unrepaired or incompletely repaired cyanotic congenital heart disease, including those with palliative shunts and conduits
- a completely repaired congenital heart defect with prosthetic material or device, whether placed by surgery or by catheter intervention, during the first six months after the procedure
- any repaired congenital heart defect with residual defect at the site or adjacent to the site of a prosthetic patch or a prosthetic device
- a cardiac transplant that develops a problem in a heart valve.
ถ้าดูจาก regiment ของปี 2007 แล้วจะเห็นว่าพวก VSD ASD ไม่ต้องให้ antibiotic prophylaxis เนื่องจากพวกนี้ถือเป็น congenital heart disease แบบไม่เขียว (non-cyanotic)
มันมีเหตุผลที่พิจารณาเปลี่ยน regiment ก็คือ underlying disease ที่ผู้ป่วยมีนั้นเมื่อเกิด IE แล้วถึงแก่ชีวิตหรือไม่ อย่าง Mitral value prolapse โอกาสเกิด IE ก็สูงพอสมควรแต่ว่าเมื่อเกิดแล้วไม่ถึงแก่ชีวิต แต่ถ้าเป็น Artificial heart values นั้นถ้าเกิด IE แล้วโอกาสเสียชีวิตมีสูง ดังนั้น regiment ใหม่จึงให้ไม่ต้องให้ prophylaxis ในผู้ป่วย MVP
แต่ก็มีข้อควรระวังที่ว่าถ้าผู้ป่วยมีโรคอื่นร่วมด้วย เช่น เบาหวาน ไตวาย ภูมิคุ้มกันไม่ดี โอกาสที่จะเสียชีวิตเมื่อมีการเกิด IE ก็จะสูงมากขึ้น
อีกเหตุผลที่ทำให้เปลี่ยน regiment เพราะว่า evidence base research มันไม่ได้ให้ผลที่เด่นชัดว่าการให้ prophylaxis มันป้องกัน IE ได้จริงหรือไม่ ควรจะไปป้องกันในการส่งเสริม oral health มากกว่า เนื่องจากถ้า oral health ไม่ดีแค่การ แปรงฟัน flossing ก็ทำให้เกิด IE ได้แล้ว
และการให้ Antibiotic เกินความจำเป็นยังทำให้เกิดการดื้อยาของ bacterial และผลข้างเคียงอื่นๆ
ก่อนจ่าย antibiotic ใดๆก็ควรพิจารณาถึงข้อดี ข้อเสีย ก่อนที่วันหนึ่งจะไม่มียา antibiotic ให้ใช้รักษาเนื่องจาก bacteria มันดื้อยาหมดแล้ว
08 April 2008
BSSO(Bilateral sagittal split osteotomy) VIDEO CLIP
เอา Clip BSSO(Bilateral sagittal split osteotomy) มาฝาก
11 February 2008
Nerve injury
การบาดเจ็บของเส้นประสาท(Nerver injury)ที่แบ่งโดย Seddon ในปี 1943 แบ่งได้เป็นสามแบบ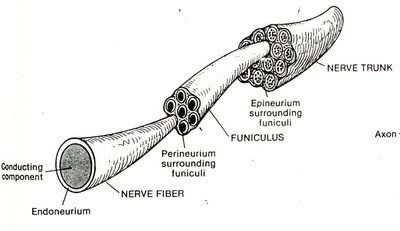
- Neurapraxia คือ เป็นอาการบาดเจ็บที่รุนแรงน้อยที่สุด ส่วนใหญ่มักเกิดเส้นประสาทโดนกด ทำให้การนำสัญญาณของเส้นประสาทเสียไป เมื่อหายดีแล้วก็จะส่งสัญญาณประสาทได้ตามปกติ การบาดเจ็บแบบนี้ไม่ทำให้เกิด degeneration
- Axonotmesis คือ การขาดของ axon (nerve fiber) โดยที่ endoneurium ยังไม่ขาดออกจากกัน การบาดเจ็บแบบนี้จะทำให้สูญเสียความรู้สึก และไม่สามารถบังคับอวัยวะให้เคลื่อนไหวได้ แต่การบาดเจ็บแบบนี้ยังสามารถหายได้ เนื่องจาก endoneurium ยังอยู่ axon สามารถงอกใหม่ไปตาม endoneurium ได้
- Neurotmesis คือการขาดของเส้นประสาท โดยที่ endoneurium ก็ขาดไปด้วย การบาดเจ็บแบบนี้เป็นการบาดเจ็บที่รุนแรงที่สุด แก้ไขได้ด้วยการผ่าตัดเท่านั้น
05 February 2008
Localized teeth with radiopraph (x-ray)
One method to localized teeth(object) in dental radiograph is SLOB rule.
SLOB is shorten from Same Lingual Opposite Buccal.
Let take a look at the picture below to explain this rule.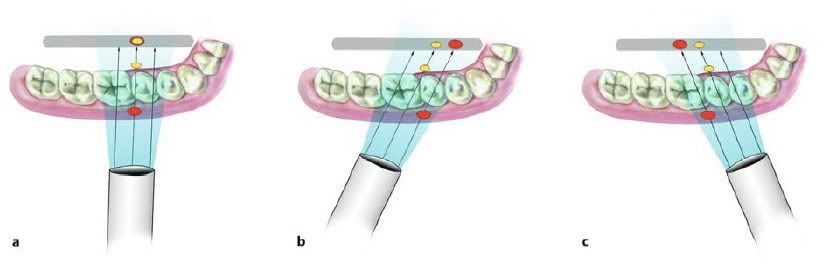
The object at lingual site will move in the same direction of the x-ray tube, opposing to the buccal object.
This rule also works in vertical dimension.
03 February 2008
Maxillary Fracture
- Fracture Zygoma (Tripod Fracture) น่าจะเป็น fracture ที่เกิดขึ้นมากที่สุดในบรรดา fracture of facial bone pattern ของ fracture มักจะเกิดจาก direct blow to body of zygoma จากการตรวจจะพบเห็นลักษณะของ contour abnormalities,มีอาการของ extraocular muscle entrapped (คือมี limitation of eye movement ในบางทิศทาง) และ force ที่มาจากทาง lateral wall of orbit อาจส่งผลไปถึง orbital apex ,optic canal เกิด diminish vision ได้ ,นอกจากนั้นการ displace ไปของ zygoma อาจไปกีดกัน motion of mandible
ส่วนในภาพรังสี x-ray โดยเฉพาะใน water’s view จะเห็น discontinuity lines of Dolan และแน่นอนครับ ผู้เขียนแนะนำว่า CT จะช่วยการ diagnosis ได้ดีมาก
- Fracture Zygomatic arch pattern of fracture นั้นเกิดจากมีแรงมากระทำทางด้านข้างของ ใบหน้า ลักษณะของใบหน้านั้นจะพบว่ามี flatness of lateral cheek area and inability to open mouth อันเนื่องมาจากการที่ zygomatic arch fragment ลงมาขัดขวางการเคลื่อนที่ของ coronoid process และ temporalis muscle ส่วนภาพรังสีที่ใช้ในการ diagnosis ได้ดีคือ view submentovertex

- Fracture of Alveolar process of Maxilla เกิดขึ้นกับ small piece of maxilla ร่วมกับมี several fracture teeth สำหรับข้อ comment เกี่ยวกับ x-ray นั้นมีอยู่ว่าในกรณีที่สงสัย film chest x-ray จะช่วยในการตรวจสอบว่ามีการ aspirate foreign body หรือ tooth fragment ลงไปใน airway หรือไม่
- Orbital floor fracture , or “Blowout” fracture mechanism ของ fracture ก็คือว่า มีแรงหรือวัตถุมากระแทกรอบๆบริเวณดวงตา แล้วส่งแรงผ่าน soft tissue กระจายไปรอบๆดวงตาและผ่านมายัง thin floor of orbit เกิดการ fracture floor orbit และมี dropdown of orbital content to maxillary sinus
clinical sign ที่พบได้ก็คือ enophthalmos and diaplopia ส่วนใน film Water’s view จะพบเงาของ soft tissue mass บริเวณ superior margin of maxillary sinus หรืออาจจะเห็น trapdoor fragment of bone protruding down to sinus
- Fracture Nose โดยปกติแล้วเราสามารถเห็น fracture นี้ได้จาก standard lateral skull film แต่ถ้าเราใช้ technique low kVp ใน x-ray ก็จะสามารถเห็น บริเวณ fracture นั้นและ soft tissue ได้ดีขึ้น แต่ก็ต้องระวังการดู film ผิดพลาดคือเห็น normal suture line หรือ linear channel for Nasociliary nerve เป็น fracture line ได้เหมือนกันนะครับ เราควรจะดูใน lateral film ที่มีแนวรังสีตั้งฉากกับ nose จะทำให้เห็น fracture line ที่มักจะเป็นแนวตั้งฉากกับ nasal bridge ได้ชัดเจนกว่า

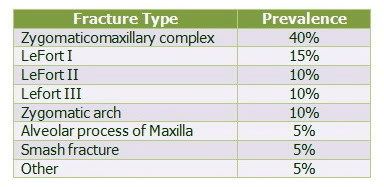
- LeFort fracture หรือเป็น fracture ที่ complex bilateral fractures associated with large unstable fragment and invariably involve pterygiod plates โดยแนวของ fracture นั้นแบ่งเป็น 3 ระดับคือ
- LeFort I มีแนว Fracture ตาม transmaxillary plane
- LeFort II มีแนว fracture ตาม subzygomatic หรือ pyramidal plane ที่มี apex บริเวณ nasal bridge
- LeFort III มีแนว fracture ตาม craniofacial plane
- Smash Fracture มีการคิดคำนี้ขึ้นมาเพื่อใช้เรียก severe comminution of the face with underlying skull injuries และยังรวมไปถึง fracture facial bone ที่ไม่สามารถ classified ไว้ในกลุ่มที่ผ่านๆมาได้ โดยรวมไปถึง Fracture frontal ,naso-ethmoidal ,naso-frontal ซึ่ง Fracture ในกลุ่มนี้ควรใช้ CT ในการตรวจจะได้รายละเอียดที่ดีกว่า plain film ทั่วไป
6.1 LeFort I หรือ tranmaxillary fracture มีแนวหัก ไปตาม maxillary floor & orbital floor โดย involve medial & lateral walls of maxillary sinuses และทางด้านหลัง involve pterygoid plate of sphenoid bone จะพบลักษณะ floating maxilla
6.2 Lefort II หรือ เรียกตามแนวทางของ fracture line ว่า Pyramidal fracture ลักษณะของ fracture นี้หลังจากมีแรงในแนวตรงเข้าด้านหน้ามากระทำแล้วจะมี mechanism ที่ downward below to nasal area
6.3 LeFort III เป็น most severe ของ LeFort fracture ลักษณะจะเป็น Large unstable(floating) fragment ทั่วไปทั้งใบหน้า หรือเรียกตามอาการว่า Craniofacial disassociation
Relate links
Diagnosis Image Facial Fracture
Mandibular fracture
Mandibular fracture

Mandible นั้นถือเป็น prominent position ที่มักเกิดการบาดเจ็บได้ง่าย ในสมัยก่อน นั้นมีอุบัติการณ์ประมาณ 2:1 เมื่อเทียบกับ facial bone fracture อื่นๆ แต่หลังจากมี high speed automobile accident มากขึ้น อุบัติการณ์ก็มาใกล้เคียงกัน โดย fracture mandible มี Clinical sign ทั่วๆไปหลายอย่างเช่น facial distortion, malocclusion, abnormal mobility, stepping formation เป็นต้น
โดยปกติแล้วเราถือ fracture mandible อยู่ใน” Ring bone rule” คือกระดูกที่มีลักษณะโค้ง ดังนั้นเมื่อเรา เห็นแนว fracture แห่งหนึ่งจากการตรวจหรือจากภาพรังสีก็ตามทีแล้ว ก็มีโอกาสสูงที่เราจะพบ fracture อีกแห่งหนึ่งในmandible ด้านตรงกันข้าม เนื่องจากลักษณะการกระจายแรงที่มากระทำของกระดูก mandible นี้ นอกจากนั้นยังมีปัจจัยการมี flexibility ของ รูปร่าง mandible รวมไปถึง การ absorb แรงโดย TMJ
จากกฎข้างต้น Fracture mandible นั้นจึงอาจเกิดเป็น double fractures ได้เช่น bilateral sides of symphysis ,combination include angle mandible plus contralateral body or condyle ส่วน triple fracture นั้นก็อาจเกิดขึ้นได้เช่น fracture both condyle and symphysis ครับ
สุดท้ายมีข้อคิดแถมอยู่ใน website นะครับ - Wise saying about Mandibular fracture
- คำนึงถึง “Ring bone Rule” เอาไว้
- Panoramic film นั้นนับเป็น single film ที่ใช้ตรวจดู fracture mandible ได้ดีมาก
- สังเกตโดยรอบของ cortical margin of mandible เพื่อหา discontinuities( fracture line) line
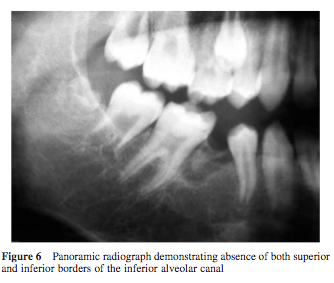
- อย่าลืมสังเกตดูว่ามี discontinuities of inferior alveolar canal หรือไม่
- Fracture line ที่ผ่าน root นั้นเรานับเป็น open fracture
- Mandibular Fractures นั้นยังมีสาเหตุหลายอย่างที่มากกว่า trauma เช่น Pathologic fracture นั้นสามารถเกิดขึ้นได้ จาก ทั้ง tumor, infection เช่น osteomyelitis
Relate links
Diagnosis Image Facial Fracture
Maxillary fracture
29 January 2008
Diagnosis Image Facial Fracture
กระดูกบริเวณใบหน้านั้นมีความซับซ้อนค่อนข้างมาก การที่เราจำเป็นต้องตรวจผู้ป่วยที่ได้รับบาดเจ็บในบริเวณนี้นั้นจึงเป็นเรื่องไม่ง่ายนัก การรู้เพียงแค่ normal anatomy ของบริเวณนี้นั้นคงไม่พอเพียงเราจำเป็นต้องรู้ลึกไปถึง common facial fracture pattern อีกด้วย สำหรับบทความนี้ผู้เขียนได้บรรยายถึงการตรวจวินิจฉัย fracture ของกระดูกใบหน้าและ ขากรรไกร โดยเน้นไปที่การใช้ภาพรังสีในการตรวจ
สำหรับตัวผู้เขียนแล้วในสถาบันของเขาใช้ CT Scan ในการตรวจ fracture of Maxillofacial region เพื่อดูทั้ง hard +soft tissue (บ้านเราคงเอาอย่างเขายาก) ส่วน indication ในการใช้ plain film นั้นมีน้อยลงเรื่อยๆโดยมีการใช้ใน case ที่มี focal trauma เช่น Fracture nose แต่อย่างไรก็ตามผู้เขียนก็ยังเห็นความสำคัญของ plain film facial series ที่เราใช้เป็นพื้นฐานในการศึกษา normal anatomy และ Fracture pattern ในขั้นเริ่มต้นก่อนจะไปดู CT ใน plain ต่างๆ
Basic Facial series ประกอบด้วย 3-4 film คือ Water’s view(PA view with cephalad angulation) ,Caldwell’s view(PA view), Lateral view และ Submentovertex view ที่ได้ใช้ในบางโอกาส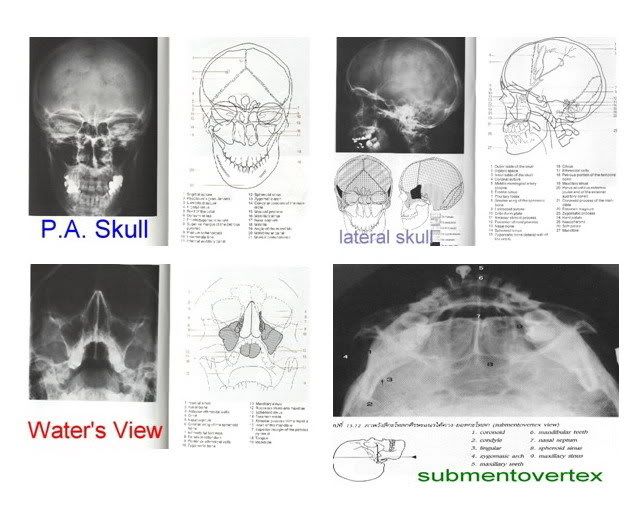
เอาละครับเมื่อถ่าย Film ต่างๆนี้มาแล้วก็มาถึงขั้นตอนการแปลผลหรืออ่าน film กันโดยมีกฎง่ายๆที่ผู้เขียนแนะนำไว้ดังนี้
- มองไปที่ Orbit ทั้งสองข้าง 60-70% ของ Facial fractures มักจะ involve orbit ด้วยแล้วแต่ว่าจะมากหรือน้อย จะมีที่ไม่มายุ่งกับ orbit ก็พวก fracture pure nasal bone ,fracture zygomatic arch, Lefort I fracture ฉนั้นอย่าลืมดูที่ orbit ให้ดีตั้งแต่ใน apex หรือ optic canal ออกมายัง orbital rim
- ข้อนี้บอกว่าเราต้องมีความรู้เกี่ยวกับ Facial fracture patterns เพื่อจะได้มีแนวในการสอดส่ายตา มองหาจุดที่หัก
- ใช้หลักการของการเปรียบเทียบ ซ้ายกับขวา เพราะมีหลักการที่เป็นความจริงเป็นภาษาอังกฤษที่ว่าใน Normal radiopacities are usually bilateral, while abnormal ones are usually unilateral
- ตรวจแนวเส้นรังสีของกระดูก Lines of Dolan จาก film Water’s view
Line of Dolan คือ เส้นในภาพรังสี ที่แสดง three anatomic contours ผ่าน facial important structure

หลังจากดูตามหลัก 4 ข้อไปแล้วเราก็เริ่มสังเกต Radiographic signs of Facial fractures กันต่อครับ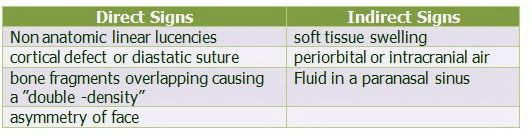
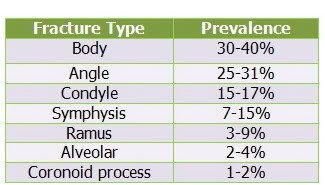
ตารางแสดง Most common patterns of midfacial fractures
(เป็น series ของ web แห่งนี้เท่านั้นนะครับ )
Article from http://www.geocities.com/omfsesan/facialfracture.htm
Relate links
Maxillary Fracture
Mandibular Fracture
28 January 2008
Oral and Maxillofacial Surgery Secrets, 2nd Edition
By A. Omar Abubaker, DMD, PhD and Kenneth J. Benson, DDS Oral and Maxillofacial Surgery Secrets, 2nd Edition written in the question-and-answer style of the successful The Secrets Series®, the latest edition of Oral and Maxillofacial Surgery Secrets presents all of the most current clinical aspects of oral and maxillofacial surgery, including maxillofacial trauma, diagnosis of salivary gland disease, cysts and tumors, postoperative care, cleft lip and palate, oral and maxillofacial reconstruction, laser surgery, facial alloplastic implants, sleep apnea, and much, much more. The new edition has been completely updated by a diverse and distinguished group of contributors, and reflects recent advances in the field. More details (1)
Oral and Maxillofacial Surgery Secrets, 2nd Edition written in the question-and-answer style of the successful The Secrets Series®, the latest edition of Oral and Maxillofacial Surgery Secrets presents all of the most current clinical aspects of oral and maxillofacial surgery, including maxillofacial trauma, diagnosis of salivary gland disease, cysts and tumors, postoperative care, cleft lip and palate, oral and maxillofacial reconstruction, laser surgery, facial alloplastic implants, sleep apnea, and much, much more. The new edition has been completely updated by a diverse and distinguished group of contributors, and reflects recent advances in the field. More details (1)
Peterson’s Principles of Oral and Maxillofacial Surgery book, second edition
 Peterson’s Principles of Oral and Maxillofacial Surgery, Second Edition, encompasses a wide range of diverse topics making it a unique text amongst the medical and dental specialties. The purpose of this concise, easy-to-read two-volume text is to provide an authoritative and currently referenced survey of the specialty of Oral and Maxillofacial Surgery. It contains the necessary information for clinicians and is an ideal reference text for preparation for board certification in the specialty.
Peterson’s Principles of Oral and Maxillofacial Surgery, Second Edition, encompasses a wide range of diverse topics making it a unique text amongst the medical and dental specialties. The purpose of this concise, easy-to-read two-volume text is to provide an authoritative and currently referenced survey of the specialty of Oral and Maxillofacial Surgery. It contains the necessary information for clinicians and is an ideal reference text for preparation for board certification in the specialty.
Expansions to the Second Edition include:
- anesthesia section to encompass comprehensive patient assessment and management in the peri-anesthetic period.
- osseointegrated implant section to include chapters on soft and hard tissue adjunctive procedures, zygomaticus and novum systems, as well as a section on implant prosthodontics for the surgeon.
- new chapters on cleft orthodontics and distraction osteogenesis. Read more detail.
VOLUME ONE Part I . Principles of Medicine, Surgery, and Anesthesia
1. Wound Healing 2. Medical Management 3. Perioperative Management 4. Preoperative Patient Assessment 5. Pharmacology of Outpatient Anesthesia Medications 6. Pediatric Sedation Part 2. Dentoalveolar Surgery 7. Management of Impacted Teeth Other than Third Molars 8. Impacted Teeth 9. Preprosthetic Surgery 10. Osseointegrated Implants 11. Adjunctive Soft Tissue Implant Procedures 12. Adjunctive Hard Tissue Implant Procedures 13. Zygomaticus and Novum Systems 14. Implant Prosthodontics Part 3. Maxillofacial Infections 15. Principles of Management of Odontogenic Infections 16. Sinus Infections 17. Osteomyelitis/Osteoradionecrosis/HBO Part 4. Maxillofacial Trauma 18. Initial Patient Assessment 19. Soft Tissue Injuries 20. Rigid vs. Semi-Rigid vs. Non-Rigid Fixation 21. Dentoalveolar Trauma 22. Mandible and Condylar Fractures 23. Maxillary and Zygomaticomaxillary Complex Fractures 24. Ocular and Orbital Trauma 25. Management of Fractures of the Frontal Sinus Fractures and Naso-orbito-ethrnoid Complex 26. Gunshot Injuries 27. Pediatric Maxillofacial Trauma 28. Management of Panfacial Fractures Part 5. Maxillofacial Pathology 29. Differential Diagnosis of Oral Disease 30. Odontogenic Cysts and Tumors 31. Benign Nonodontogenic Lesions of the Jaws 32. Head and Neck Cancer: Diagnosis, Classification, Staging 33. Oral Cancer: Treatment 34. Lip Cancer 35. Salivary Gland Disease and Tumors 36. Management of Mucosal and Related Dermatologic Disorders 37. Skin Cancer
VOLUME TWO Part 6. Maxillofacial Reconstruction
38. Local and Regional Flaps 39. Bony Reconstructions 40. Microvascular Free Tissue Transfer 41. Microneurosurgery 42. Cleft Lip and Palate 43. Alveolar Cleft Grafting 44. Secondary & Adjunctive Cleft Procedures 45. Craniofacial Syndromes 46. Craniosynostosis Part 7. Temporomandibular Joint Disease 47. TMJ Anatomy and Pathophysiology 48. Non-Surgical Management 49. Arthrocentesis / Arthroscopy 50. Surgery for Internal Derangements of the Temporomandibular Joint 51. Management of the End-Stage TMJ Patient 52. Hypomobility and Hypermobility Part 8. Orthognathic Surgery 53. Growth and Development 54. Quantification and Visualization of the Surgical Patient Problem-Based Diagnosis and Treatment Planning 55. Orthodontics For Orthognathic Surgery 56. Mandibular Surgical Procedures 57. Maxillary Surgical Produces 58. Management of Facial Asymmetry 59. Esthetic Soft Tissue Changes in Orthognathic Surgery 60. Prevention and Management of Complications of Orthognathic Surgery 61. Cleft Management in Orthognathic Surgery 62. Distraction Osteogenesis 63. Surgical and Nonsurgical Management of Obstructive Sleep Apnea Part 9. Facial Esthetic Surgery 64. Blepharoplasty 65. Rhinoplasty 66. Rhytidectomy 67. Forehead and Brow Procedures 68. Liposculpting Procedures 69. Skin Rejuvenation Procedures 70. Alloplastic Esthetic Facial Augmentation 71. Otoplastic Surgery for the Protruding Ear
22 January 2008
The art of a good suture
I was given a very gracious gift today: A pair of large needle drivers! For what purpose? To learn how to suture of course. The needle driver has other names as well. Some call them hemostats - although I am not sure if this is technically correct. According to the website atitan.com (the manufacturer of my new gift) they are called needle holders and my size is an M7. Here is a photo:

The M7 stands for mayohegar 7′. These things also have a carbide tip. Well, this has peaked my interest in suturing so I have been doing some research for everyone. This will tell you how to get your own things to start learning how to suture. What you will need:
- A guide to help you know how to tie the knots: Ethicon down loadable manual or if that link doesn’t work e-mail me and I can e-mail you the one I downloaded.
- Needle holders, or needle drivers: Visit your local OR office or hospital surgical floor and ask for ‘old ones’ . Surgical departments constantly renew their stash and may have some. Make sure to explain clearly that it is for educational experiance and that you are a student.
- A knot tying board or suture practice board: Again visit the local hospital or look on the internet. Some resources are Ethicon and other suture companies. If this option is not available you can call Johnson & Johnson and ask for a free Ethicon knot tying board, rope, and a knot tying manual. The number is 1-800-255-2500. The items will ship within 7-10 days.
- Sutures or string. I have read that some hospitals will get rid of expired sutures or you can find them online for a reduced price. Rope or string works just as well though to get the techniques down. The feel will be different between twine, yarn, string, and a silk suture, although the method is still the same. Keep this in mind. Repeating the same knot over and over again with a two foot long suture will last a while, so you don’t need much.
The first thing I was taught was how to palm the needle drivers and open and close them using both my dominant and non dominant hand. I am right handed, so I will show this method first:
It is fairly simple to open and close the needle driver with your hands in the finger loops, so I will skip to the non-loop technique, which is used more often in surgery because it allows you to have better rotational and free movement of the instrument and your hand. Try to take your hand in and out of the finger loops rapidly while twisting and turning. It is difficult and palming the whole instrument is better. I have read online of directors wanting to see proficiency in both skills though, so bear this in mind. The first thing to do is hold the instrument almost like you would a marshmallow roaster.

Do you see how my fingers are holding down tightly on the bottom half of the instrument. Note that the needle driver is in a closed position. Now using some force while holding steady with your fingers, push the pad of your hand (below the thumb - see where the needle driver is resting in the palm?) against the needle holder so it clicks open. Practice this many times on the three different closed positions and practice rotating the instrument along its long axis in your hands 180 degrees or more when the needle holder is closed and then open it up again after spinning it.
After a suture is done, it needs to be cut. With talking to an experienced oral surgeon I learned that when you are good you can hold both the needle driver and scissors in one hand and flip back and forth with each one to suture and then cut, suture and then cut. I don’t have scissors, but I will show you how to fling the instrument out of the way to free up your hand. I am sure this has to be seen in surgery to be appreciated. One reason shadowing is a must before making this a career goal.
Hold the instrument like shown above but place your ring finger in the bottom loop. After practicing a couple of sutures you will then fling the needle drivers toward your body while using your ring finger as a pivot for the needle holder.

The needle driver will go from the above picture to the below picture:

Pretty cool how it frees up your hand right? You can now use scissors to cut the suture AND you can use the scissors in the same hand. To get the needle driver back up into your palm, use a small wrist twitch along with the muscle of your pinky (in a motion that clenches the pinky) to fling it back up. It takes some practice to get it down and it will take longer to master. It is useful to do this while studying or reading. It can be done in lecture where no note taking is required. It can also be done in your white coat pocket while walking around. The oral surgeon I shadow would practice during his anesthesia rotation by tying a suture off onto one of the many cords coming off the anesthesia carts and suturing away.
The non dominant hand I find is more difficult. I am left handed. This method is done mostly with the fingers and thumb, minus the palm. A picture speaks 1000 words so I will let you look and explain afterwards:

See the pressure I am able to put on the needle driver with the fingers pushing in one direction snd the tumb pushing towards the fingers? This is enough to open the needle holder and it still provides a good grip on the instrument to open and close it.
Practice all of these methods using all the needle holder locking positions. Rapidly open and close the instrument several times and then close it and spin it (rotate the instrument along its long axis) a couple of times and then open it and close it several times more. The reason you spin the needle driver is because most needles are curved in a half circle shape and a spinning motion is required to drive the needle into the tissue and then back out again.
These are the basics. Don’t hesitate to ask a surgeon to demonstrate some of these techniques to you. Most surgeons will be proud to show off their skills! Stay tuned for demonstrations of knot tying with easy to follow instructions so you can tie like the best!
Article from http://omfsource.com/blog/2007/08/03/the-art-of-a-good-suture/What is a Oral and maxillofacial surgeon??
An oral and maxillofacial surgeon is a regional specialist surgeon treating the anatomical area of the mouth, jaws, face, skull, as well as associated structures.
Oral & maxillofacial surgeons are usually initially qualified in dentistry and have undergone further surgical training. Some OMS residencies integrate a medical education as well & an appropriate degree medicine (MBBS or MD or equivalent) is earned, although in the United States there is legally no difference in what a dual degree OMFS can do compared to someone who earned a four year certificate. Oral & maxillofacial surgery is universally recognized as a one of the nine specialties of dentistry. However also in the UK and many other countries OMFS is a medical specialty as well culminating in the FRCS (Fellowship of the Royal College of Surgeons). Regardless, all oral & maxillofacial surgeons must obtain a degree in dentistry (BDS, BDent, DDS, or DMD or equivalent) before being allowed to begin residency training in oral and maxillofacial surgery.
They also may choose to undergo further training in a 1 or 2 year fellowship to expand the scope of practice to areas such as:
- Head and neck cancer - microvascular reconstruction
- Cosmetic facial surgery
- Craniofacial surgery/Pediatric Maxillofacial surgery
- Cranio-maxillofacial trauma
The popularity of oral and maxillofacial surgery as a career for persons whose first degree was medicine, not dentistry, seems to be increasing. Integrated programs are becoming more available to medical graduates allowing them to complete the dental degree requirement in about 3 years in order for them to advance to subsequently complete Oral and Maxillofacial surgical training.
[edit] Surgical procedures
Treatments may be performed on the mouth, jaws, neck, face, skull, and include:
- Dentoalveolar surgery (surgery to remove impacted teeth, difficult tooth extractions, extractions on medically compromised patients, bone grafting or preprosthetic surgery to provide better anatomy for the placement of dentures or other dental prostheses)
- Diagnosis and treatment of benign pathology of the region (cysts, tumors etc.)
- Diagnosis and treatment (ablative and reconstructive surgery) of malignant pathology of the region (oral & head and neck cancer)
- Diagnosis and treatment of cutaneous malignancy (skin cancer)
- Diagnosis and treatment of congenital craniofacial malformations such as cleft lip and palate and cranial vault malformations such as craniosynostosis, (craniofacial surgery)
- Diagnosis and treatment of chronic facial pain disorders
- Diagnosis and treatment of temporomandibular joint (TMJ) disorders
- Diagnosis and treatment of dysgnathia (incorrect bite), and orthognathic (literally "straight bite") reconstructive surgery, orthognathic surgery, Maxillomandibular advancement
- Diagnosis and treatment of soft and hard tissue trauma of the oral and maxillofacial region (jaw fractures, cheek bone fractures, nasal fractures, skull fractures and eye socket fractures.
- Splint and surgical treatment of sleep apnea, Maxillomandibular advancement (in conjunction with sleep labs or physicians)
- Surgery to insert osseointegrated (bone fused) dental implants or Maxillofacial implants for attaching Craniofacial prosthesis.
- Cosmetic surgery limited to the head and neck (Rhytidectomy/facelift, Blepharoplasty, Otoplasty, Rhinoplasty, Genioplasty, etc.)
A well known example of a facial trauma case was the reconstruction of Trevor Rees-Jones's face, which was literally flattened by the impact of the car crash that killed Diana, Princess of Wales. Dr Luc Chikhani rebuilt the shattered facial bones, working from photographs, and implanting hundreds of titanium screws and brackets.
In November 2005 Isabelle Dinoire became the first person in the world to receive a face transplant.[2] The procedure was completed by Dr Bernard Devauchelle a French oral and maxillofacial surgeon at Amiens University Hospital.
Article from http://en.wikipedia.org/wiki/Oral_and_maxillofacial_surgery
13 January 2008
Vasovagal Syncope and dental consideration
วันนี้อ่านใน satabun พบ keyword คำหนึ่งว่า vasovagal syncope
คงต้องแยกสองคำนี้ออกจากกันก่อน
Syncope คือการเป็นลมหมดสติไปในช่วงระยะเวลาสั้น เรียกอีกอย่างหนึ่งว่า fainting
Vasovagal มาจาก vagus nerve หรือ nerve X นั้นเอง
รวมกันแล้ว vasovagal syncope คือการหมดสติไปเนื่องจาก vagus nerve นั้นเอง
แล้ว vagus nerve ทำให้หมดสติได้อย่างไร คงต้องรู้กันก่อนว่า vagus nerve ทำหน้าที่อะไร vagus nerve มีส่วน motor ที่กระตุ้น parasympathetic ไปยังเกือบจะทุกอวัยวะในร่างกาย และอวัยวะที่สำคัญที่สุดก็น่าจะเป็นหัวใจนั้นเอง
น่าจะรู้กันอยู่แล้วว่า Parasympathetic จะทำให้หัวใจเต้นช้าลง หลอดเลือดขยายตัว ซึ่งส่งผลให้ cardiac output ลดลง blood pressure ลดลง ซึ่งอาจส่งผลให้เลือดไปเลี้ยงสมองไม่พอ ทำให้วิงเวียน หน้ามืด เป็นลม หมดสติ
ทุกคนน่าจะเคยมีประสบการณ์ที่นอนบนเตียงแล้วลุกขึ้นอย่างรวดเร็ว ทำให้เกิดอาการหน้ามืด ต้องล้มลงไปนอนต่ออีกสักพักอาการหน้ามืดก็หายไป นี้ก็เพราะเวลาเราลุกอย่างรวดเร็ว เลือดมันตามขึ้นไปเลี้ยงสมองไม่ทัน เมื่อเรานอนลงเลือดก็กลับมาเลี้ยงสมองได้ ทำให้รู้สึกดีขึ้น
อีกตัวอย่างหนึ่งคือ การยืนเป็นเวลานานๆ แล้วหน้ามืด วิงเวียง ก็เพราะเลือดไหลลงไปอยู่ส่วนล่างของร่างกายหมด ทำให้ขึ้นไปเลี้ยงสมองไม่พอ
ตัวอย่างทั้งสองก็คือการกระตุ้น vagus nerve จนอาจทำให้เกิด vasovagal syncope นั้นเอง ส่วนว่าทำไมเมื่อเกิดเหตุการณ์เหล่านี้แล้ว ร่างกายจึงต้องไปกระตุ้น vagus nerve ให้เป็นลมนั้นจริงๆแล้วเป็นกระบวนการป้องกันอันตรายที่อาจจะเกิดขึ้นกับร่างกาย ลองคิดถึงเหตุการณ์ที่ยกตัวอย่างมาทั้งสองแล้วเราไม่เป็นลมลงไป สมองก็จะตายเพราะขาดเลือดได้
ยังมีสาเหตุที่ทำให้เกิด vasovagal syncope ได้อีก เช่น ความเครียด(stress) ความเจ็บปวด การเสียเลือดมาก การเห็นเลือด(การเห็นเลือดสำหรับบางคน จะทำให้ร่างกายคิดว่าตัวเองเสียเลือดมากทำให้เกิดการกระตุ้น vasovagal syncope ได้
Dental consideration
การป้องกันการการเกิด vasovagal syncope ในการรักษาทางทันตกรรม ก็คือ การลดความเจ็บปวด ทำให้คนไข้เครียดน้อยที่สุด อย่าให้ผู้ป่วยเสียเลือดมาก
แล้วถ้าเกิด vasovagal syncope ละต้องทำอย่างไร ก็หยุดทำฟัน เอาทุกอย่างออกจากปาก ให้นอนราบยกขาสูง ประเมิน ABC ให้ดมแอมโมเนีย ให้ Oxygen ถ้าในหนึ่งนาทียังไม่ฟื้นเรียก EMS ได้เลย
คงได้ประโยชน์กันบ้าง ไม่มากก็น้อย
Reference
- ทำไมบางคนที่ยืนนานๆ หรือเห็นหยดเลือดจึงเป็นลมได้? http://www.bloggang.com/viewdiary.php?id=duen&month=11-2006&date=23&group=7&gblog=206
- Pocket guide to medical emergencies in the dental office, LCDR V.C. LAPOINTE, DC, USN
Diabetes Mellitus drug with dental consideration
Adrenal insufficiency and Dental consideration
10 January 2008
Diabetes Mellitus drug with dental consideration
คงมีทันตแพทย์หลายๆคนไม่รู้ว่ายาที่ใช้รักษาโรคเบาหวานมีอะไรบ้าง และมีผลอย่างไรกับทางทันตกรรม มารู้จักยาที่รักษาเบาหวานตามตารางกันก่อน ที่ใช้กันบ่อยมีแค่ไม่กี่ตัว จำไม่ยาก
Drug used in Diabetes Mellitus
| DRUG CLASS | GENERIC (TRADE) DRUG NAMES* | MECHANISM OF ACTION |
| Sulfonylureas | Chlorpropamide (Diabinese) Glipizide (Glucotrol) Glyburide (DiaBeta, Micronase) Glimepiride (Amaryl) | Stimulate insulin secretion |
| Meglitinides | Repaglinide (Prandin) | Stimulate insulin secretion |
| Biguanides | Metformin (Glucophage) | Decrease glycogenolysis and hepatic glucose production |
| Alpha-Glucosidase Inhibitors | Acarbose (Precose) Miglitol (Glyset) | Decrease gastrointestinal absorption of carbohydrates |
| Thiazolidinediones | Rosiglitazone maleate (Avandia) Pioglitazone (Actos) | Enhance tissue sensitivity to insulin |
ที่คุ้นๆกันก็คือ MF ก็คือ Metfomin ให้รู้แล้วกันว่า MF คือตัวย่อของ Metformin เวลาเจอคนไข้เบาหวานจะได้ไม่งงว่ากินยาอะไรอยู่ ยาในกลุ่มนี้เท่าที่รู้ไม่มีผลกับการรักษาทางทันตกรรม
กับยาในอีกกลุ่มคือ Sulfonylurea ที่คุ้นกันคือ Gliclazide, Glipizide, Glibenclamide จำง่ายๆพวก Gli ทั้งหลายนี้เอง ยากลุ่มนี้มีความสำคัญกับการรักษาทางทันตกรรมบ้างเหมือนกัน เพราะทำหน้าที่กระตุ้นให้เกิดการหลั่ง Insulin ออกมามาก ถ้าผู้ป่วยได้รับการรักษาในช่องปากแล้วทำให้ไม่สามารถทานข้าว ทานอาหารได้เหมือนเดิม ก็อาจจะทำให้เกิดภาวะ Hypoglycemia ได้
ยากลุ่มหนึ่งที่ไม่ได้รักษาโรคเบาหวานโดยตรงแต่เป็นการป้องกัน Complication ที่จะเกิดกับโรคเบาหวาน ก็คือ Aspirin โดยแพทย์แต่ละคนก็จะให้ Dose ต่างๆกันไปแล้วแต่เรียนหรือเชื่อกันมายังไง แต่จะให้เป็น low dose คือตั้งแต่ 75-325 mg (Grain I 65mg, Grain V 325mg) Aspirin มีผลกับการทำงานศัลยกรรมในช่องปากคือ ทำให้เลือดหยุดยากขึ้น โดยทันแพทย์จะถูกสอนกันมาให้หยุด ASA 7 วันก่อนการถอนฟันในช่องปาก แต่จากการศึกษาในปัจจุบันทำให้ ADA บอกว่าไม่ต้องหยุด ASA ในการทำ minor oral surgery เอาเป็นว่าถอนฟันไม่เกิน 3 ซี่แล้วกัน อย่างไรก็ตามควรจะซักประวัติ ตรวจร่างกายด้านอื่นๆของผู้ป่วยประกอบด้วย และควรจะมีสารห้ามเลือดพร้อม เช่น Gelfoam หรือ Surgicel
หวังว่าคนอ่านคงได้ประโยชน์จากเกร็ดความรู้เรื่องยาในการรักษาโรคเบาหวานบ้างครับ
หมายเหตุ: ผู้ป่วยเบาหวานมีความเสี่ยงจากการเสียชีวิตด้วย cardiovascular event, myocardial infarction, stroke เพิ่มขึ้น 2-4 เท่า ทั้งผู้ชายและผู้หญิง
Reference
- Brennan, Michael T. DDS, MHS a; Wynn, Richard L. PhD b; Miller, Craig S. DMD, MS c. Aspirin and bleeding in dentistry: an update and recommendations; Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, & Endodontics. 104(3):316-323, September 2007.
- RAJESH V. LALLA, B.D.S., Ph.D.; JOSEPH A. D’AMBROSIO, D.D.S., M.S. Dental management considerations for the patient with diabetes mellitus, JADA, Vol. 132, October 2001
- http://www.student.chula.ac.th/~45350858/appirin.html
Relate link
Vasovagal Syncope and dental consideration
Adrenal insufficiency and Dental consideration
Adrenal insufficiency and Dental consideration
การเกิด adrenal insufficiency เกิดได้จากการรับ exogenous steroid ทำให้สมดุลของ Hypothalamus-pituitary-adrenal gland (HPA-axis)เสียไป
ในภาวะปกติร่างกายจะหลั่ง cortisone ประมาณ 50 mg/day
ถ้ามีความเครียดจะหลั่งมากขึ้นเป็น ประมาณ 75 mg/day
ถ้าต้องทำหัตถการเช่นการ ผ่าตัด จะมีการหลั่งเพิ่มเป็น 200-500 mg/day
ดังนั้นผู้ป่วยที่มี adrenal insufficiency จะทำให้ไม่สามารถหลั่ง cortisone ได้เพียงพอกับความต้องการของร่างกาย โดยจะมีลักษณะอาการดังนี้ คือ blood pressure ลดลง, ซึม, Hypoglycemia, เป็นลม
วิธีการสังเกตว่าคนไข้รับยา steroid เป็นเวลานาน ดูได้จากลักษณะดังนี้
- หน้าจันทร์แรม (moon face)
- แกมอ้อยเชื่อม (hyperglycemia)
- เอื้อมไม่ไหว (แขนขาลีบ)
- ยายมีหนวด (ผู้หญิงมีหนวด)
- ลายหน้าท้อง (หน้าท้องแตก)
- ปวดกระดูก
- ลูกทะเล (Na retention ทำให้บวมน้ำ)
- เท่ห์เหมือนควาย (buffalo hump ลักษณะที่มี fat สะสมอยู่ตามคอและหลัง)
- ถิ่นเรดเซลล์ (จำนวนเม็ดเลือดแดงผิดปกติ)


เมื่อใดจะเกิด adrenal insufficiency
1. การได้รับ prednisolone มากกว่า 5 mg/day เป็นเวลา 3 อาทิตย์ จะทำให้เกิด adrenal insufficiency เป็นเวลา 1 ปี
2. การได้รับยาพ่น steroidในการรักษา asthma
เมื่อใดไม่เกิด adrenal insufficiency
- รับ steroid น้อยกว่า 3 อาทิตย์
- Prednisolone น้อยกว่า 5 mg/day นานเท่าใดก็ได้
Dental consideration in adrenal insufficiency patient
- Minor surgery เช่น ถอนฟัน ขูดหินปูน ถ้าคนไข้หยุดกิน steroid แล้วก็ให้กิน dose เท่าที่เคยกินถ้ายังกินอยู่ก็ไม่ต้องให้เพิ่ม
- Moderate stress เช่น ผ่าฟันคุด ตัดกระดูก ตัดชิ้นเนื้อ ให้ double dose ที่คนไข้เคยกินแล้ว taper dose ลงหรือให้ 50mg IV ก่อนผ่าตัด จากนั้นให้ 25mg IV q8h for 24hr
Vasovagal syncope and dental consideration
Diabetes Mellitus drug with dental consideration
Subscribe to:
Posts (Atom)
